




























The most common causes of back pain are diseases of the spine, mainly degenerative-dystrophic (osteochondrosis, deforming spondylosis) and over-tension of the back muscles. In addition, various diseases of the abdominal cavity and small pelvis, including tumors, can cause the same symptoms as a herniated disc, compressing the spinal root.
It is no coincidence that these patients turn not only to neurologists, but also to gynecologists, orthopedists, urologists and above all, of course, to district or family doctors.
Etiology and pathogenesis of low back pain
According to modern concepts, the most common causes of lower back pain are:
- pathological changes in the spine, mainly degenerative-dystrophic;
- pathological changes in muscles, most often myofascial syndrome;
- pathological changes in the abdominal organs;
- diseases of the nervous system.
The risk factors for low back pain are:
- intense physical activity;
- uncomfortable working posture;
- injury;
- cooling, drafts;
- alcohol abuse;
- depression and stress;
- occupational diseases associated with exposure to high temperatures (especially in hot stores), radiation energy, with strong temperature fluctuations, vibration.
Some of the spinal causes of lower back pain include:
- root ischemia (discogenic radicular syndrome, discogenic radiculopathy), resulting from compression of the root by a herniated disc;
- reflex muscle syndromes, which can be caused by degenerative-dystrophic changes in the spine.
A certain role in the occurrence of back pain can be played by various functional disorders of the lumbar spine, when blocks of intervertebral joints appear due to poor posture and their mobility is impaired. In the joints above and below the block, compensatory hypermobility develops, resulting in muscle spasms.
Signs of acute compression of the spinal canal
- numbness in the perineal area, weakness and numbness in the legs;
- delay in urination and bowel movements;
- with compression of the spinal cord, a decrease in pain is observed, alternating with a feeling of numbness of the pelvic girdle and limbs.
Lower back pain in childhood and adolescence is most often due to abnormalities in the development of the spine. Non-proliferation of the vertebral arches (spina bifida) occurs in 20% of adults. The examination reveals hyperpigmentation, birthmarks, multiple scars and hyperkeratosis of the skin in the lumbar region. Sometimes there is urinary incontinence, trophic disorders, weakness in the legs.
Lower back pain can be caused by lumbarization - the transition of the S1 vertebra from the lumbar spine - and sacralization - the attachment of the L5 vertebra to the sacrum. These anomalies are formed due to the individual features of the development of transverse processes of the vertebrae.
Nosological forms
Almost all patients complain of back pain. The disease is mainly manifested by inflammation of the sedentary joints (intervertebral, costo-vertebral, lumbosacral joints) and ligaments of the spine. Gradually, ossification develops there, the spine loses its elasticity and its functional mobility, becomes like a bamboo stick, fragile, easily injured. At the stage of pronounced clinical manifestations of the disease, the mobility of the chest during breathing and, as a result, the vital capacity of the lungs significantly decreases, which contributes to the development of a number of lung diseases.
Tumors of the spine
Distinguish benign tumors from malignant tumors, mainly of spinal and metastatic origin. Benign spinal tumors (osteochondroma, chondroma, hemangioma) are sometimes clinically asymptomatic. With hemangioma, a vertebral fracture can occur even with small external influences (pathological fracture).
Malignant tumors, mostly metastatic, originate in the prostate, uterus, breast, lungs, adrenal glands, and other organs. Pain in this case is much more common than in benign tumors - usually persistent, painful, aggravated by the slightest movement, depriving patients of rest and sleep. Characterized by a gradual deterioration of the condition, an increase in general exhaustion, pronounced changes in the blood. Radiography, computed tomography, magnetic resonance imaging are of great importance for diagnosis.
Osteoporosis
The main cause of the disease is a decrease in the function of the endocrine glands due to an independent disease or against the background of the general aging of the body. Osteoporosis can develop in patients who take hormones for a long time, chlorpromazine, anti-tuberculosis drugs, tetracycline. Radicular disorders accompanying back pain result from a deformation of the intervertebral foramen and spine (myelopathy) - due to compression of the radiculomedullary artery or a vertebral fracture, even after minor injuries.
Myofascial syndrome
Myofascial syndrome is the main cause of back pain. It can occur as a result of overwork (during intense physical exertion), excessive stretching and bruising of the muscles, non-physiological posture during work, reactions to emotional stress, shortening of a leg and even of flat feet.
Myofascial syndrome is characterized by the presence of so-called "trigger" areas, on which pressure causes pain, often radiating to neighboring areas. In addition to myofascial syndrome, inflammatory muscle diseases - myositis can also cause pain.
Low back pain often occurs with diseases of internal organs: gastric ulcer and duodenal ulcer, pancreatitis, cholecystitis, urolithiasis, etc. They can be pronounced and mimic the image of lumbago or discogenic lumbosacral radiculitis. However, there are also clear differences, thanks to which it is possible to differentiate reflected pain from those resulting from diseases of the peripheral nervous system, which are due to the symptoms of the underlying disease.
Clinical symptoms of low back pain
Most often, low back pain occurs between the ages of 25 and 44. Distinguish acute pain, which usually lasts 2-3 weeks and sometimes up to 2 months. , And chronic - more than 2 months.
Radicular compression syndromes (discogenic radiculopathy) are characterized by a sudden onset, often after carrying heavy loads, sudden movements, hypothermia. Symptoms depend on the location of the lesion. At the heart of the syndrome is the compression of the root by a herniated disc, which occurs as a result of dystrophic processes, facilitated by static and dynamic loads, hormonal disturbances, trauma (including microtrauma to the spine). Most often, the pathological process involves areas of the vertebral roots from the dura mater to the intervertebral foramen. In addition to the herniated disc, bone growths, scar changes in epidural tissue, and an enlarged yellow ligament may be involved in trauma to the root.
The upper lumbar roots (L1, L2, L3) rarely suffer: they do not represent more than 3% of all lumbar radicular syndromes. Twice as often, the L4 root is affected (6%), causing a characteristic clinical picture: slight pain along the inner-inferior and anterior aspect of the thigh, on the medial aspect of the leg, paresthesia (sensation ofnumbness, crawling) in this area; mild quadriceps weakness. Knee reflexes persist and sometimes even increase. The L5 root is most often affected (46%). The pain is localized in the lumbar and gluteal regions, along the outer surface of the thigh, the antero-outer surface of the lower leg to the foot and III-V fingers. It is often accompanied by a decrease in the sensitivity of the skin of the antero-external surface of the leg and the strength of the extensor digitorum III-V. It is difficult for the patient to stand on the heel. With long-term radiculopathy, hypotrophy of the anterior tibialis muscle develops, and the S1 root is often affected (45%). In this case, the pain in the lower back radiates along the outer-posterior surface of the thigh, the outer surface of the lower leg and the foot. The examination often reveals hypalgesia of the postero-external surface of the leg, a decrease in the strength of his triceps and flexors of the toes. It is difficult for these patients to stand on their toes. There is a decrease or loss of the Achilles reflex.
Vertebral lumbar reflex syndrome
It can be acute and chronic. Acute low back pain (LBP) (lumbago, "lumbago") occurs within minutes or hours, often suddenly due to awkward movements. Throbbing, stabbing pain (like an electric shock) is localized throughout the lower back, sometimes radiates to the iliac region and buttocks, sharply increases with coughing, sneezing, decreases when lying down, especially if the patient finds acomfortable position. Movement in the lumbar spine is limited, the lumbar muscles are tense, the symptom of Lasegue is provoked, often bilateral. Thus, the patient is lying on his back with the legs extended. The doctor simultaneously flexes the affected leg at the knee and hip joints. This does not cause pain, because in this position of the leg the diseased nerve is relaxed. Then the doctor, leaving the leg bent in the hip-hip joint, begins to unfold it in the knee, causing strain on the sciatic nerve, which causes severe pain. Acute lumbodynia usually lasts 5 to 6 days, sometimes less. The first attack ends faster than the following ones. Recurrent attacks of lumbago tend to progress to chronic PB.
Atypical back pain
There are a number of atypical clinical symptoms for back pain caused by degenerative-dystrophic changes in the spine or myofascial syndrome. These signs include:
- the onset of pain in childhood and adolescence;
- back injury shortly before the onset of lower back pain;
- back pain with fever, or signs of intoxication;
- spine;
- rectum, vagina, both legs, pain in the girdle;
- the link between lower back pain and eating, defecation, intercourse, urination;
- obituary pathology (amenorrhea, dysmenorrhea, vaginal discharge), which arose against the background of back pain;
- increased pain in the lower back in a horizontal position and a decrease in a vertical position (Razdolsky's symptom, characteristic of the tumor process of the spine);
- steadily increasing pain for one to two weeks;
- limbs and the appearance of pathological reflexes.
Survey methods
- external examination and palpation of the lumbar region, detection of scoliosis, muscle tension, pain and trigger points;
- determination of the range of motion in the lumbar spine, areas of muscle wasting;
- search for neurological condition; determination of symptoms of tension (Lassegh, Wasserman, Neri). Study of Wasserman's symptom: flexing the knee in a prone patient causes pain in the hip. Study of the symptom of Neri: a sharp tilt of the head towards the chest of a patient lying on the back with the legs straight, causes sharp pain in the lower back and along the sciatic nerve. ];
- study of the state of sensitivity, reflex sphere, muscle tone, autonomic disorders (swelling, changes in color, temperature and humidity of the skin);
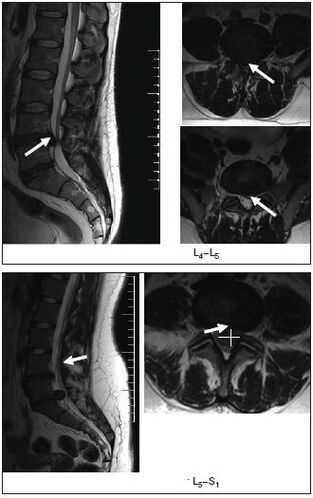
- x-ray, magnetic resonance or computerized imaging of the spine.
MRI is particularly informative.
- ultrasound examination of the pelvic organs;
- gynecological examination;
- if necessary, additional studies are carried out: cerebrospinal fluid, blood and urine, sigmoidoscopy, colonoscopy, gastroscopy, etc.
Treatment
Acute low back pain or exacerbation of vertebral or myofascial syndromes
Undifferentiated treatment. Soft motor mode. With severe pain the first few days, rest in bed, then walk with crutches to relieve the spine. The bed should be firm, a wooden board should be placed under the mattress. For warmth, a woolen shawl, electric heating pad, heated sand or salt bags are recommended. Ointments have a beneficial effect: finalgon, tiger, capsin, diclofenac, etc. , as well as mustard plasters, pepper plaster. Ultraviolet irradiation recommended in erythematous doses, leeches (taking into account any contraindications), irrigation of the painful area with ethyl chloride.
The anesthetic effect is provided by electrical procedures: percutaneous electroanalgesia, sinusoidal modulated currents, diadynamic currents, novocaine electrophoresis, etc. The use of reflexology (acupuncture, laser, moxibustion) is effective; blocking of novocaine, pressure massage of the trigger points.
Drug therapy includes pain relievers, NSAIDs; tranquilizers and / or antidepressants; medicines that reduce muscle tension (muscle relaxants). In the event of arterial hypotension, tizanidine should be prescribed with great caution due to its hypotensive effect. If swelling of the spinal roots is suspected, diuretics are prescribed.
The main analgesics are NSAIDs, which are often used uncontrollably by patients when the pain gets worse or comes back. It should be noted that long-term use of NSAIDs and pain relievers increase the risk of complications from this type of therapy. Currently, there is a large selection of NSAIDs. For patients with pain in the spine, in terms of availability, effectiveness and less likelihood of side effects (gastrointestinal bleeding, dyspepsia), diclofenac 100-150 mg / day is preferable to "no" drugs. selective ". inside, intramuscularly, rectally, topically, ibuprofen and ketoprofen within 200 mg and topically, and "selectively" - meloxicam within 7. 5-15 mg /day, nimesulide within 200 mg / day.
In the treatment of NSAIDs, side effects may occur: nausea, vomiting, loss of appetite, pain in the epigastric region. Possible ulcerogenic action. In some cases, there may be ulceration and bleeding in the gastrointestinal tract. In addition, headache, dizziness, drowsiness, allergic reactions (rash, etc. ) are noted. Treatment is contraindicated in ulcerative processes of the gastrointestinal tract, pregnancy and lactation. To prevent and reduce dyspeptic symptoms, it is recommended to take NSAIDs with or after meals and to drink milk. In addition, taking NSAIDs with increased pain in combination with other drugs that the patient takes to treat concomitant diseases, leads, as observed with long-term treatment of many chronic diseases, to a decreaseadherence to treatment and, consequently, insufficient efficacy of therapy.
Therefore, modern methods of conservative treatment include the obligatory use of drugs with a chondroprotective, chondrostimulating effect and having a better therapeutic effect than NSAIDs. These requirements are fully met by the drug Teraflex-Advance, which is an alternative to NSAIDs for mild to moderate pain syndrome. One capsule of the drug Teraflex-Advance contains 250 mg of glucosamine sulfate, 200 mg of chondroitin sulfate and 100 mg of ibuprofen. Chondroitin sulfate and glucosamine are involved in the biosynthesis of connective tissue, helping to prevent the destruction of cartilage, stimulating tissue regeneration. Ibuprofen has analgesic, anti-inflammatory and antipyretic effects. The mechanism of action is due to the selective blockade of cyclooxygenase (COX type 1 and type 2) - the main enzyme in the metabolism of arachidonic acid, which leads to a decrease in the synthesis of prostaglandins. The presence of NSAIDs in the preparation Teraflex-Advance helps to increase the range of motion of the joints and to reduce morning stiffness in the joints and spine. It should be noted that, according to R. J. Tallarida et al. , The presence of glucosamine and ibuprofen in Teraflex-Advance ensures synergy with regard to the analgesic effect of the latter. In addition, the analgesic effect of the glucosamine / ibuprofen combination is provided by 2, 4 times the dose of ibuprofen.
After relieving the pain, it is reasonable to switch to taking Teraflex, which contains the active substances chondroitin and glucosamine. Teraflex is taken 1 capsule 3 times a day. during the first three weeks and 1 capsule twice a day. in the next three weeks.
In the overwhelming majority of patients, when taking Teraflex, there is a positive trend in the form of relief from the pain syndrome and a decrease in neurological symptoms. The drug is well tolerated by patients, no allergic manifestations were noted. The use of Teraflex in degenerative-dystrophic diseases of the spine is rational, especially in young patients, both in combination with NSAIDs and as monotherapy. In combination with NSAIDs, the analgesic effect is twice as fast and the need for therapeutic doses of NSAIDs is gradually reduced.
In clinical practice, for lesions of the peripheral nervous system, including those associated with osteochondrosis of the spine, B vitamins with neurotropic effects are widely used. Traditionally, the method of alternating administration of vitamins B1, B6 and B12, 1-2 ml is used. intramuscularly with daily alternation. The duration of treatment is 2 to 4 weeks. The disadvantages of this method include the use of small doses of drugs which reduce the effectiveness of the treatment and the need for frequent injections.
For discogenic radiculopathy, traction therapy: traction (including underwater) is used in a neurological hospital. In case of myofascial syndrome after local treatment (blockage of novocaine, irrigation with ethyl chloride, anesthetic ointments), a warm compress is applied to the muscles for several minutes.
Chronic low back pain of vertebrogenic or myogenic origin
In the event of a herniated disc, it is recommended:
- wear a rigid corset of the "weight lifting belt" type;
- elimination of sudden movements and inclinations, limitation of physical activity;
- physiotherapy exercises to create a muscle corset and restore muscle mobility;
- massage;
- blockade of novocaine;
- reflexology;
- physiotherapy: ultrasound, laser therapy, heat therapy;
- intramuscular vitamin therapy (B1, B6, B12), multivitamins with mineral supplements;
- for paroxysmal pain, carbamazepine is prescribed.
Non-drug treatments
Despite the availability of effective means of conservative treatment, the existence of dozens of techniques, some patients require surgical treatment.
Indications for surgical treatment are divided into relative and absolute. An absolute indication for surgical treatment is the development of caudal syndrome, the presence of a sequestered herniated disc, a pronounced radicular pain syndrome, which does not decrease, despite ongoing treatment. The development of radiculomyeloischemia also requires urgent surgery. However, after the first 12-24 hours, the surgical indications in such cases become relative, on the one hand due to the formation of irreversible changes in the roots and, on the other hand, because in most cases in AuDuring treatment and rehabilitation, the process regresses in about 6 months. The same periods of regression are observed with deferred transactions.
Relative indications include ineffectiveness of conservative treatment, recurrent sciatica. The duration of conservative treatment should not exceed 3 months. and last at least 6 weeks. It is assumed that the surgical approach in case of acute radicular syndrome and ineffectiveness of conservative therapy is justified within the first 3 months. after the onset of pain to prevent chronic pathological changes in the root. A relative indication is cases of extremely pronounced pain syndrome, when the pain component changes with an increase in neurological deficit.
From physiotherapeutic procedures, electrophoresis with the proteolytic enzyme caripazime is currently widely used.
It is known that physiotherapy and massage are an integral part of the complex treatment of patients with spinal injuries. Therapeutic gymnastics pursues the objectives of general strengthening of the body, increasing efficiency, improving coordination of movements, improving physical condition. At the same time, special exercises are aimed at restoring certain motor functions.